INGROWN TOENAIL TREATMENT
This is all about ingrown toenails, ingrown toenail treatment, ingrown toenail removal, and all sorts of ingrown toenail facts.
Podiatrist in Las Vegas House / Hotel Call Fees
Painful, Ingrown Toenail
This is all about ingrown toenails- ingrown toenail treatment, ingrown toenail removal, and all sorts of ingrown toenail facts. Some of this information you may find useful while other parts not so much. If you have any questions please feel free to send me an email.
There are multiple nail pathologies. An ingrown nail maybe referred simply as onychocryptosis (photo right on top). Paronychia describes an acute infectious process (photo above on right), typically from bacteria S. aureus. A myxoid cyst is a translucent, dome- shaped solitary nodule commonly over the distal interphalangeal joint. With nail trauma we somteimes see a subungual hematoma. There are many differential diagnoses for subungual hematoma such as glomus tumor, Kaposi sarcoma, melanoma, exostosis, melonychia striata, and keratoacanthomas. It is best to biopsy the nail if uncertain. Lacerations may also occur with trauma of the nail bed forming a hematoma. If the nail is painful or greater than 25% hematoma then often the nail is removed. Removal of nail allows for one to inspect the nail bed for deeper laceration or fracture to the underlying bone may be present.


Call Today to Schedule an Appointment
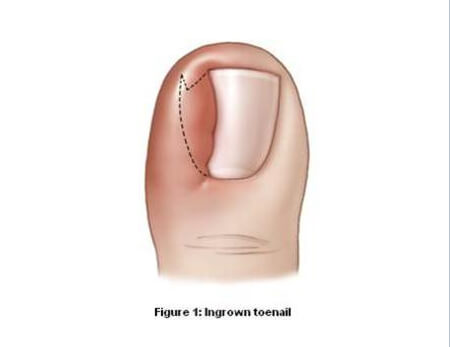
702 - 518 - 1862In terms of preventing ingrown nails, one thing I always recommend to patients is to trim the nail straight across. Cutting at an angle makes it easier for the nail to grow into the skin causing an ingrown toenail. As you can see in figure 1 that if you do cut at an angle there is sometimes residual nail at the corner that forms a spicule. Often this spicule is missed in the cutting process and grows and grows until it’s tenting the skin and the patient is in agonizing pain. Upon removal it is easy to see just how deep the spicule was (photo above). Once it reaches this point the patient should see a podiatrist so the ingrown toenail can be removed under local anesthesia as it can become infected.
Pyogenic Granuloma
There are many nail unit tumors. The most common I see is what’s called a pyogenic granuloma. It is a benign granlomatous lesion that is seen after minor trauma. These can be highly vascular so I recommend soaking the foot in warm water or epsom salt to help relieve the pain. A podiatrist will usually remove this under local anesthesia and may use silver nitrate sticks to help stop the bleeding (photo below).
A glomus tumor is a small red or bluish spot visible through the nail plate. It presents with an intense pulsating pain with pressure or exposure to cold. It consists of the afferent arteriole and efferent venule, glomus cells, smooth muscle cells, and non and myelinated nerves. A subungual exostosis is another thing we often see though it is not a tumor. It is a painful outgrowth of healthy bone but it important to differientate from something such as an osteochondroma. Subungual exostosis is often removed in the operating room by the podiatrist. Other nail unit tumors included squamous cell carcinoma, melanoma, basal cell carcinoma. Though they are rare in the toenail, they can be fatal if not treated (Bob Marley died from Acral Lentiginous melanoma of his toe).
Bowen’s disease is squamous cell carcinoma in situ and presents as one or more red, scaly, flat patches that may be up to several centimeters wide. “In situ” means that the malignant cells are confined to the epidermis. This disease can persist as such or may develop into invasive squamous cell carcinoma that is slow growing with an insidious onset.


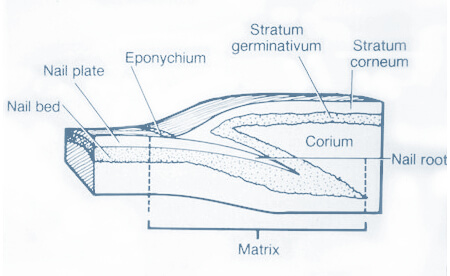
The toenail consists of many parts. As mentioned often in this website, the nail matrix is what synthesizes the nail plate substance and extends proximally 5 to 10mm in depth. This matrix is what is destroyed or removed when a podiatrist is doing a matrixectomy, which I will talk about later. The growth rate of a toenail is 0.03mm to 0.05mm a day, a slower rate then the fingernails as the toenails are further from the blood pumping heart than the fingers. The thickness of the nail is between 0.05mm and 1.0 mm. There are many arterial branches from the digital arteries of the toe, including the dorsal branches, lateral digital artery, distal and proximal arches. Innervation of the hallux is important to know as a podiatrist as these nerves are blocked during a hallux block for an ingrown toenail. These nerves include the digital branch of the deep peroneal nerve, medial dorsal cutaneous nerve, medial digital nerve from the medial plantar nerve, and the lateral common digital nerve from the medial plantar nerve.
There are many surgical options in the management of an ingrown toe nail. Many include physical removal of the matrix. Many different procedures have been proposed for doing a removal of the matrix such as the Zadik, Whitney, Frost, and Winograd, but honestly these are rarely done. As a resident we took all our ingrown nails to the operating room which is a bit silly to me. The reason for this was because the hospital didn’t allow us to use Phenol for the matrixectomy (atleast while I was there). Phenol is an acid and yes it sometimes may cause a phenol burn but the majority of patients do just fine. Otherwise one can instead use sodium hydroxide instead of phenol which is shown to be a safer alternative with faster healing time. When we did remove the matrix during residency we did so in the operating room under sterile conditions as you do actually go down to bone during the procedure. A dedicated office procedure room would be fine but we didn’t have one. Believe it or not removing the matrix with a 15 blade or beaver blade for ingrown toenails is a relatively difficult procedure unless you are well trained. The matrix is tiny and you need steady hands to remove it all. Sometimes the matrix comes out in pieces as the person had previous trauma. And since you are down to bone during this procedure the person must be free from infection which is tricky as many people have infection with an ingrown toenail. Long story short, I prefer chemical matrixectomies and so do most podiatrists. Chemical matrixectomies are done in an office under local anesthesia. Typically 1% or 2% Lidocaine and/or 0.25% or 0.50% Marcaine are used. Personally I do not use an epinephrine mixture when removing ingrown toenails with a matrixectomy but some do as it helps control the bleeding better which is important when doing a matrixectomy, while others believe it may cause too much constriction leading to necrosis of the nail. Bottom line is its probably fine to use just so long as you don’t have any vascularity compromise or peripheral vascular disease.
Now the injection isn’t fun. It’s similar to going to the dentist and they numb your tooth, it is a quick sharp pain and its over… some people it doesn’t bother at all while others it hurts. If your podiatrist is nice he will often spray your foot with ethyl chloride while injecting for the ingrown nail. This just causes a freezing/cold sensation to the foot to get your mind off the pain, and it works. I have my own way of numbing the toe which involves doing it in steps with an insulin needle which drastically reduces the pain. I surveyed 20 of my patients who had my special type of injection vs the traditional injection, and my injection was rated as a 3/10 on the pain scale and the traditional 7/10! It usually takes about 3-5ml of the anesthesia to numb the great toe for an ingrown toe nail, although more maybe needed if there is an infection present as this makes the anesthesia less effective. Once numbed up the patient will feel pressure but not pain. The forefoot/toe is then scrubbed either with this dark orange solution known as Betadine or another solution known as Chlorhexidine.

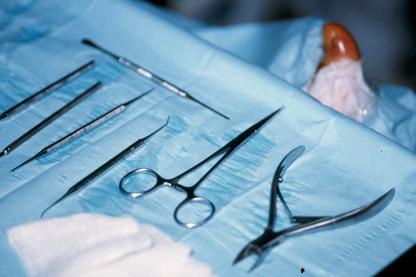
Though this is a “clean” procedure (not “sterile”) it is important to have proper prepping of the foot and sterilized equipment. Some doctors use cold sterilization which means they keep the instruments in an antiseptic solution for so many hours to sterilize the instruments. Nowadays most podiatrists (including myself) use an autoclave which is the standard of care with sterilization of instruments. Once you are numbed and prepped the podiatrist will then use the instruments to begin the procedure. The process starts by using a freer elevator or spatula to go underneath the affected portion of the nail to free the nail from the nail bed. Then an English Anvil is used to cut the nail. Now this is important, when cutting the nail the doctor has to make sure all the nail is cut. Often one thinks they cut the entire nail since they are at the base of the nail but there is sometimes a tiny piece just proximal to the nail fold which needs to be removed. Splitting the nail with the freer or spatula can help with this process. Then, using a hemostat the nail is grasped and rotated to remove the nail. The area is then inspected and a curette is used to clean any remaining remnants. Next the area is gently flushed and a dressing applied with antibiotic cream. That’s it. The patient usually keeps the dressing on for 24 hours and removes it and applies a bandaid. The patient is free to go back to work the same day though his toe will be numb for several hours. I recommend wearing sandals to the doctors appointment as sometimes the dressing is bulky and may not fit into normal shoes. The podiatrist may then ask the patient to follow up in a week or just have them call if there are any problems.

The matrixectomy is usually reserved for people who get reoccuring ingrown toenails. Some people are just more predisposed to ingrown toe nails. Take a look at your toes right now, are your nails straight? Curvy? Thick? Everyones nails are different, but chances are if you see them curving like a rainbow you are the victim of multiple ingrown toenails. Once you see a podiatrist he will do either a partial nail avulsion or a total nail avulsion. Often it is a partial nail avulsion at one of the corners where the ingrown toenail is. Only a small border/sliver of the toenail is removed as some patients think the entire toenail is removed, which isn’t true. Once the toenail is removed you may have a matrixectomy performed afterwards. Now there is an art that goes into doing the matrixectomy. Studies have shown it’s a good procedure with about a 90% success rate, meaning about 10% have another ingrown nail. But it depends on the podiatrist. For instance, is adequate hemostasis achieved? This involves exsanguination and a tourniquet as the blood will mix/flush the phenol or sodium hydroxide and interfere with the process. Another important step is how long and how many times does the podiatrist apply the acid.


Some do 3 q-tips for 30 seconds and others do 4 q-tips for 30 seconds, it varies. Also, is the phenol or sodium hydroxide expired? Again, a good podiatrist will make sure nothing is expired as this is easy to overlook. If done correctly, this is a fantastic procedure with great results.

As a 24/7 house & hotel Las Vegas Podiatrist I take pride in my thorough evaluation and treatment of toe pain and ingrown toenails. My treatment of ingrown toenails are backed by peer reviewed journals and research and in my opinion are the best treatment of ingrown toenails. I do not use “cheap” supplies and my inventory is stocked with only the most up to date and high quality supplies.
Please call now if you are around Las Vegas and suffer from heel pain, plantar fasciitis, neuroma, ingrown toenail , painful nails , warts, thick and long fungal nails, diabetic feet , or an ankle sprain. For information on what/why I use for my chemical matrixectomies for ingrown nails please visit this link.
SCHEDULE YOUR CONSULTATION