Gout TREATMENT
Gout is a common endpoint of a group of disorders that produce hyperuricemia.
Podiatrist in Las Vegas House / Hotel Call Fees
Gout
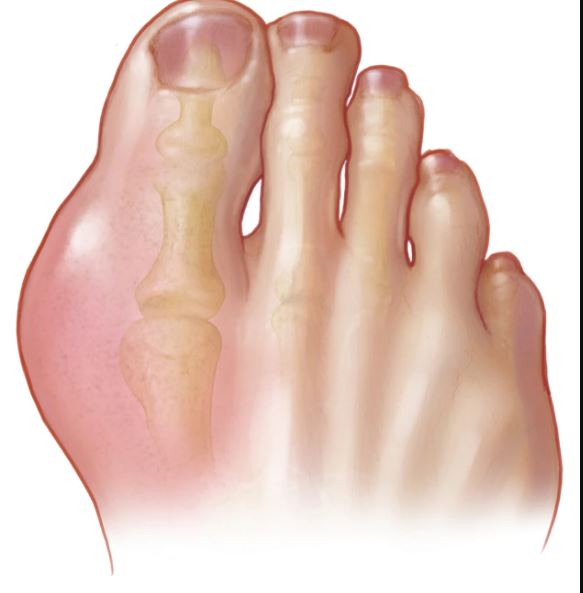
Gout is a common endpoint of a group of disorders that produce hyperuricemia. Uric acid is the final breakdown product of purine degradation in humans. Gout is a recurrent acute arthritis that affects peripheral joints, most notably the 1st MPJ (great toe joint). It is initiated by the crystallization of monosodium urate within and around joints, often eventually leading to the deposition of tophi in the surrounding tissue. These tophi consist of large aggregates of urate crystals, and the resulting immune response causes pain and inflammation. For effective treatment determination must be made as to whether the patient is an over producer of uric acid (metabolic gout) or an under excreter of uric acid (renal gout). The most common cause of gout (about 90% of cases) is the inability to excrete enough uric acid in the urine. It is important to note that not all hyperuricemic people develop gout.
Gout represents about 2-5% of all articular diseases. Factors contributing to the development of gout from hyperuricemia include: Age, genetic predisposition (enzymatic deficiencies), diet, alcohol consumption, obesity, certain drugs (ex: diuretics/Thiazides), and lead toxicity. Males are more affected than females (20:1). This Sex variation is due in part to higher functional excretion rates in females and is attributable to hormonal influences.
Call Today to Schedule an Appointment
702 - 518 - 1862The most common sign of gout is a “red, hot, swollen, painful” joint. The arthritis may become chronic and deforming. Gout classically begins in the evening or early morning and tends to occur in previously damaged joints. Diagnosis of gout includes both clinical and lab findings. Blood work is important, but not conclusively diagnostic for gout, as hyperuricemia occurs with a level greater than 7.5 mg/dl. Aspiration with crystal identification is key in a diagnosis as gout. In gout, crystals of monosodium urate (MSU) appear as needle-shaped intracellular and extracellular crystals. When examined with a polarizing filter and red compensator filter, they are yellow when aligned parallel to the slow axis of the red compensator but turn blue when aligned across the direction of polarization (ie: they exhibit negative birefringence). Negatively birefringent urate crystals are seen on polarizing examination in 85% of specimens. Microscopic analysis in pseudogout shows calcium pyrophosphate (CPP) crystals, which appear shorter than MSU crystals and are often rhomboidal. Under a polarizing filter, CPP crystals change color depending upon their alignment relative to the direction of the red compensator. Chronic gout can often appear on x-rays with “punched out” lesions, intraosseous lesions, “rat bites”, and sclerotic overhanging edges (Martel’s sign).
People with gout can’t efficiently remove excess uric acid and thus a high-purine diet may let uric acid accumulate and cause a gout attack. Research has shown that restricting high-purine foods and taking the appropriate medication can prevent gout attacks. Foods that commonly trigger gout attacks include organ meats (liver, kidney, heart, brains), red meats, seafood, lard, alcohol (especially red wine) and beer. However, there is one exception to this rule. Research shows that high-purine vegetables do not trigger gout attacks. And interestingly, fructose and sugar-sweetened beverages can increase the risk of gout and gout attacks, even though they’re not purine-rich. Instead, they may raise uric acid levels by accelerating several cellular processes. For instance, a study including over 125,000 participants found that people who consumed the most fructose had a 62% higher risk of developing gout.
Besides diet modification, there are other treatments for gout. Acute Treatments include NSAIDs (particularly Indomethacin), Colchicine (inhibits the phagocytosis of uric acid and blocks the release of chemotactic factors), and intra-articular corticosteroid injections. Chronic management often involves urate lowering drugs such as Allopurinol. Allopurinol is a hypoxanthine analogue that first acts as a substrate for xanthine oxidase, then after hydroxylation, binds to the active site of the enzyme inhibiting the formation of uric acid. A combination of Colchicine and Allopurinol are also often prescribed. In severe/advanced cases, surgical removal of tophi and even fusion of the joint maybe performed.


As a 24/7 house & hotel Las Vegas Podiatrist I take pride in my thorough evaluation and treatment of toe pain and ingrown toenails. My treatment of ingrown toenails are backed by peer reviewed journals and research and in my opinion are the best treatment of ingrown toenails. I do not use “cheap” supplies and my inventory is stocked with only the most up to date and high quality supplies.
Please call now if you are around Las Vegas and suffer from heel pain, plantar fasciitis, neuroma, ingrown toenail , painful nails , warts, thick and long fungal nails, diabetic feet , or an ankle sprain. For information on what/why I use for my chemical matrixectomies for ingrown nails please visit this link.
SCHEDULE YOUR CONSULTATION